SVT in Children
4 years old boy presents with history of difficulty in breathing , sense of fast heart beat and an episode of vomiting. On arrival to ER doctor records his heart rate of around 240/min on monitor after applying SPO2 probe, very feeble pulse and low blood pressure (70/38 mmHg). Following is the ECG of the child. What is the diagnosis and what should be the treatment steps?
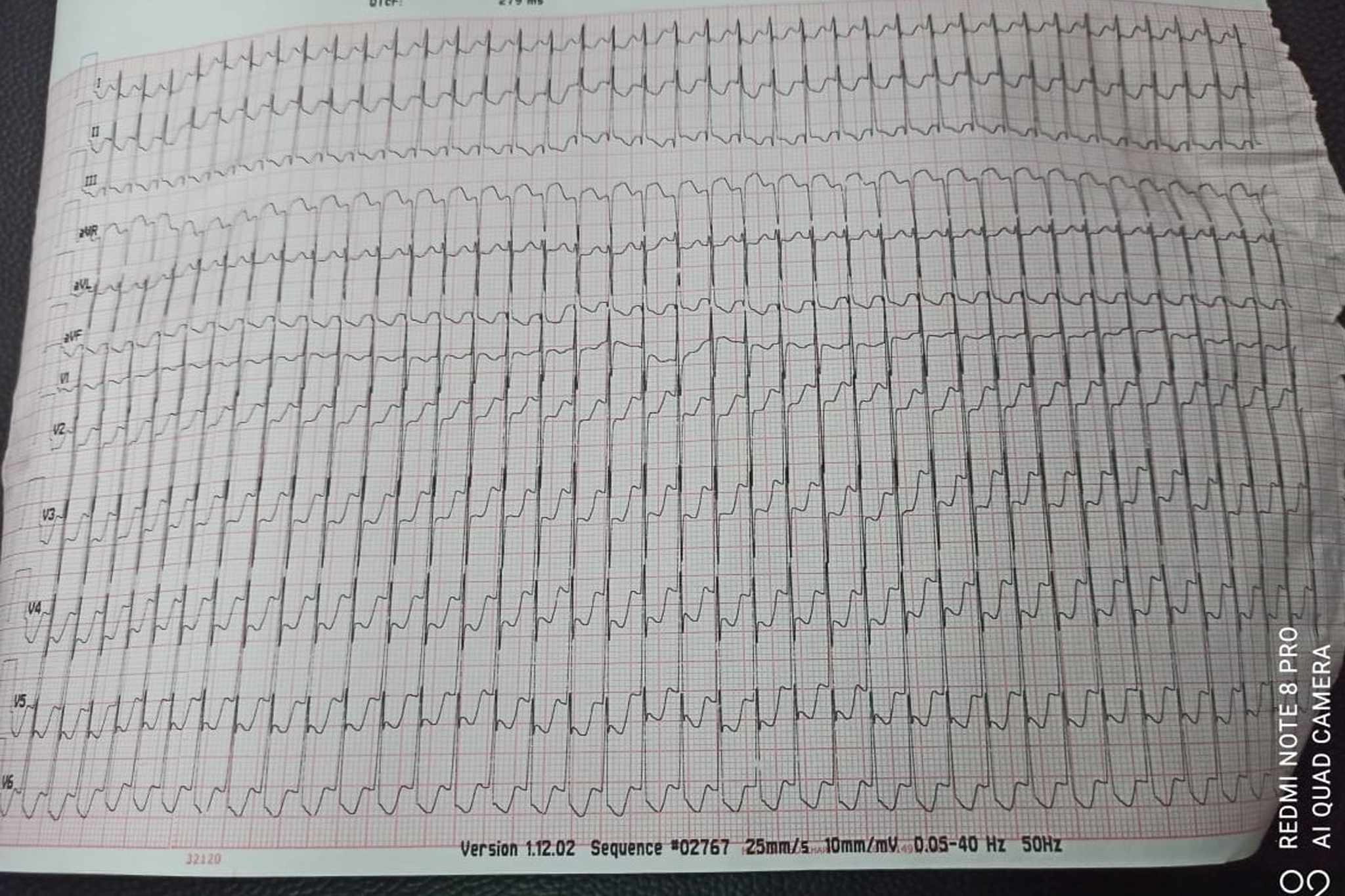
Image A , arrow showing ST segment changes
Above ECG is suggestive of supraventricular tachycardia – AVRT
Treatment steps: (only acute management )
- 12 lead ECG ,continuous ECG monitoring
- Assess for signs of cardiogenic shock ,Prolonged CRT ,Low BP ,Acidotic Blood Gas ,Gallop rhythm ,Enlarged liver
- Discuss with cardiology team early
Treatment :
- Try vagal stimulation while continuing ECG monitoring. ( vagal stimulation –mostly not effective in infants)
- ICE pack application over face
- Older children can be asked to blow forcefully through straw ( Valsalva manoeuvre)
- Adenosine :
- Intravenous adenosine (to be given rapidly into large peripheral or central vein and followed promptly by 0.9% sodium chloride flush).
- Starting dose of 100 micrograms/kg rapid flush technique , dose can be given upto 500mcg/kg (maximum 12 mg in adult) in incremental fashion at interval of 2 minutes between each dose.
- If child is unstable ( in cardiac shock -which is the case scenario mentioned here) consider for early Direct current cardio version( at 1-2 J /kg)
If there is no conversion to sinus rhythm after adenosine administration and / or DC cardio version,various other antiarrhythmic drugs can be used after consultation with cardiologist ( Amiodarone ,beta blocker, Flecainide ,Sotalol etc.)
Differentiation between sinus tachycardia and supraventricular tachycardia ( SVT) in infants and young children
| Sinus tachycardia | SVT |
|---|---|
| heart rate less than 200 per minute | Usually >220 /min |
| P waves seen ( up right in leads I and aVF leads) | P waves not easily seen , if seen it is negative in II,III and aVF leads |
| Not associated with ST segment or T wave changes | Often associated with ST segment and T wave changes ( mostly seen in cases with AVRT –atrioventricular reentry tachycardia)- commonest amongst children |
| heart rate varies from beat to beat and is often responsive to stimulation | Non variable heart rate |
| Heart rate slowly decreases in response to treatment for primary etiology ( i.e shock, sepsis) | Termination of SVT is abrupt ( either spontaneously or to treatment |